










We believe that the finger is one of the most information-rich surfaces on the human body. The photoplethysmography (PPG) sensor inside every Oura Ring continuously captures the arterial pulse wave as it travels through the finger, and hidden within that signal is a remarkably detailed picture of cardiovascular and respiratory health.
We have been investing heavily in what that signal can tell us. We are excited to share some of our recent health science findings.
What Is PPG?
Photoplethysmography (PPG) measures the volumetric changes in the arteries using light reflection.
The PPG signal is an optical measurement of the arterial pulse wave — i.e. the wave generated when blood is ejected from the heart during systole, temporarily increasing arterial pressure and causing vessel expansion and contraction. PPG works by shining a light on the finger and capturing the changes in light reflected back from the vascular bed or capillaries.
Research has shown that this signal contains a wealth of information on the heart, blood vessels, breathing, and autonomic nervous system.
Our latest PPG research spans three interconnected areas: patterns associated with hypertension, how blood pressure behaves during sleep, and breathing disturbances through the night.
PPG Patterns Associated with Hypertension
Background
High blood pressure (hypertension) is a primary driver of cardiovascular disease, yet it is often undetected or undertreated. However, “white coat hypertension,” when patients have elevated blood pressure measurements during a medical appointment but not outside of the clinical environment, occurs in 15-30% of people, and can lead to incorrect identification of high blood pressure. Our research explored whether nightly PPG data from the Oura Ring could identify physiological patterns associated with high blood pressure without a cuff. This could improve screening for hypertension at a population health level.
Research
An algorithm was developed using data from Oura’s Blood Pressure Profile Study, which as of June 2026, has enrolled more than 300,000 consenting members who contributed Oura Ring data alongside self-reported hypertension status, self-reported health information, and cuff-based blood pressure measurements.
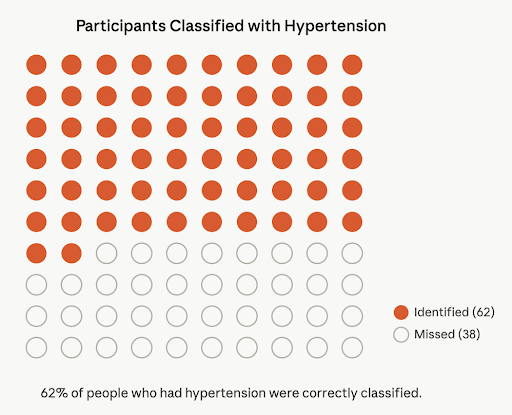
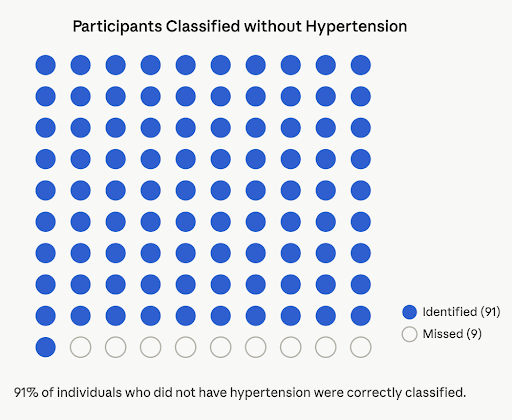
In testing, the algorithm demonstrated 62% sensitivity for detecting hypertension (1), which means that 62% of people who reported hypertension were correctly identified. The algorithm also demonstrated 91% specificity, meaning that the algorithm correctly classified 91% of individuals without known hypertension at the time of the study (2).
About Sensitivity and Specificity: Sensitivity and specificity are two key metrics used to evaluate the performance of a health screening test.
|
Overnight PPG Signals and Dipping Patterns in Blood Pressure
Background
Blood pressure should naturally dip during sleep. When it doesn’t consistently, it can be an indication of cardiovascular disease risk. Today, the standard way to measure nocturnal blood pressure dipping is ambulatory blood pressure monitoring (ABPM), a clinic-administered procedure involving a blood pressure cuff worn overnight. Because that test is not commonly used in routine care, many people with abnormal nighttime blood pressure patterns may go unnoticed.
Nighttime Blood Pressure Dipping Classifications:
|
Research
The Oura Science Team compared Oura Ring 4 PPG data with reference ambulatory blood pressure measurements in 134 participants over 48 hours to develop an algorithm to classify dippers and non-dippers. The algorithm demonstrated 84% sensitivity, meaning that it correctly identified 84% of individuals with nocturnal blood pressure dipping, and 69% specificity, meaning that it correctly identified 69% of individuals without nocturnal dipping.
The algorithm distinguished individuals with nocturnal blood pressure dipping from those without, with an Area under the Curve (AUC) of 0.87, reflecting strong discriminative ability.
By conventional benchmarks, AUC values above 0.80 are considered indicative of good classification accuracy. An AUC of 0.87 suggests that the algorithm may serve as a meaningful, non-invasive means of identifying a cardiovascular risk pattern that would otherwise require overnight ambulatory monitoring to detect.
PPG Signals and Sleep Apnea
Background
Sleep-disordered breathing encompasses a spectrum of conditions, including obstructive sleep apnea, that share a common feature: they are prevalent, underdiagnosed, and associated with significant downstream cardiovascular and cognitive risk. Current clinical screening recommendations rely on symptom reporting (snoring, daytime sleepiness, witnessed apneas) and formal polysomnography (a sleep study), both of which involve substantial barriers to access. Continuous passive monitoring of breathing patterns with wearable devices during sleep represents a complementary at-home pathway.
Research
The Oura Science Team developed an algorithm to estimate a nightly Apnea Hypopnea Index (estimated AHI, or eAHI), a count of how often breathing pauses (apneas) or shallow breathing (hypopneas) occur per hour of sleep. This metric is intended to reflect the same underlying physiology captured by the apnea-hypopnea index (AHI) used in clinical sleep medicine.
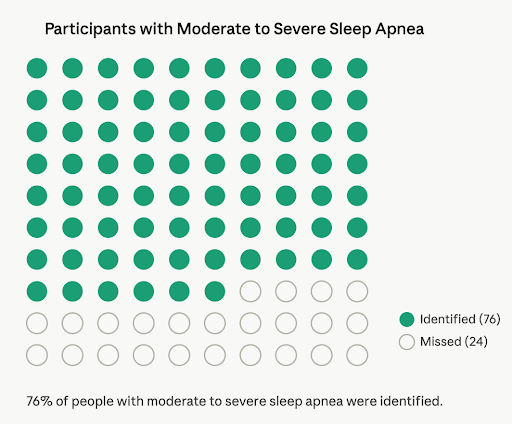
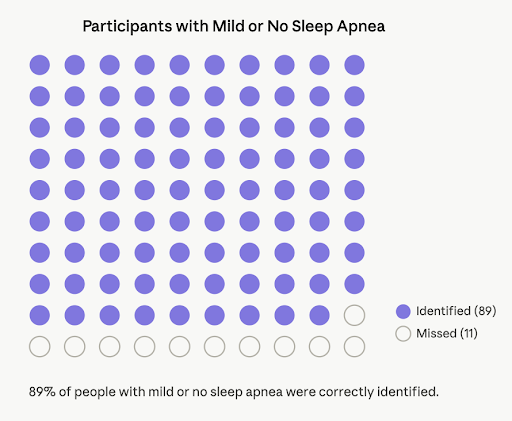
In a study of 339 participants, including 56 with diagnosed moderate to severe sleep apnea (3), the algorithm was evaluated against Type 1 attended polysomnography, the gold standard method for in-lab sleep evaluation. The algorithm showed a sensitivity of 76% for detecting moderate to severe sleep apnea, meaning that 76% of people with moderate to severe sleep apnea were correctly identified. In addition, the algorithm demonstrated a specificity of 89%, meaning that 89% of individuals with mild or no sleep apnea were correctly classified, and only 11% were incorrectly identified.
As algorithms improve and datasets grow, PPG is supporting research into areas that once required far more invasive or burdensome clinical tools. The convergence of continuous passive monitoring and large-scale population data is creating new opportunities to understand cardiovascular and respiratory health in ways that were not previously feasible outside a clinical setting.
Footnotes
(1) Hypertension was defined as: a self-reported hypertension diagnosis and average cuff BP measurements in the hypertensive range
(2) Non-hypertension was defined as: No self-report of hypertension diagnosis, not using antihypertensive medications, no cardiometabolic comorbidities and average cuff BP measurements outside the hypertensive range (when cuff measurements were available)
(3) Moderate-to-severe sleep apnea is defined as an apnea-hypopnea index (AHI)≥15, using the Center for Medicare Services (CMS) scoring rules.
Legal Disclaimer
The findings described above reflect Oura’s ongoing scientific research and are shared for the purpose of scientific dissemination. Oura Ring and the features in the Oura App are wellness products, not medical devices, and are not intended to diagnose, treat, cure, monitor, or prevent medical conditions or illnesses. Users should not make any changes to medication or other treatments without first consulting their doctor or another medical professional.